

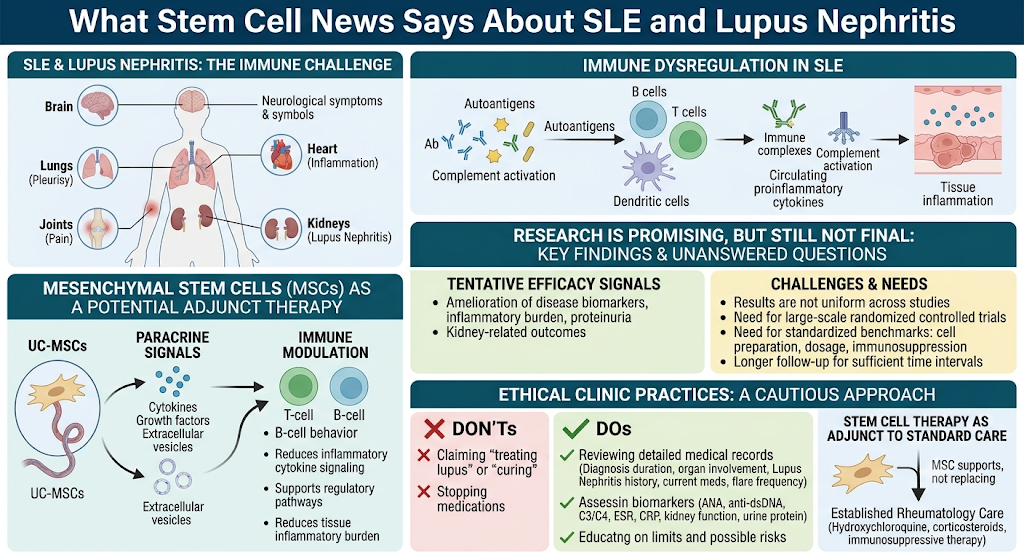
Systemic lupus erythematosus (SLE) is the most heterogeneous and complex autoimmune disease because it does not manifest uniformly across all patients. While some patients experience fatigue, joint pain, rashes, and/or photosensitivity, or recurrent flares. While a smaller number may go on to suffer from complications such as kidney involvement, blood abnormalities, neurological symptoms, or inflammation of the lining around the heart (cardiac tamponade) or lungs (pleurisy), which have also been observed in some patients with long-term organ damage.
Which is why a lot of patients are reviewing stem cell therapy Thailand and soaking up every component of stem cell news that pertains to clever autoimmune ailment. Not only are they seeking a new treatment. And they are searching for answers to help them make sense of why their immune system keeps attacking their own bodies.
The sensible response here is not at all sensational. Stem cell therapy does not assure the cure of SLE. It should not be a substitute for rheumatology care, hydroxychloroquine use, immunosuppressive medication therapy, and biologics, including monitoring the kidneys or standard management of lupus. However, mesenchymal stem cells (MSCs), especially UC-MSCs, are experimentally investigated for their immunomodulatory and anti-inflammatory signaling.
Why SLE Is More Than a Flare
Lupus Is an Immune Communication Problem
SLE results when the immune system misdirects these antibodies that it developed in response to infections or autoantigens to react against normal tissues. This can mainly consist of the role played by B cells, T cells, dendritic cell antigen that leads to autoantibodies (Ab), immune complexes and complement activation or circulating proinflammatory cytokines in peripheral circulation or at-tissue level inflammation.
This is also known as SLE; thus, it can affect multiple organs. Depending on a given patient’s disease phenotype, this response can affect the skin, joints, kidneys, blood vessels, as well as components of the nervous system and internal organs.
As patients, this is often experienced as a part of the unpredictability. One month may feel stable. The next month could also bring fatigue, swollen joints, pain and other laboratory abnormality tests or a flare secondary to an infection, stress exposure (sunlight), hormonal changes in the body [18], lack of sleep or changes in medication.
A good medical plan should not only ask, “How do we stop this flare?” It should also ask, “How do we reduce future immune overactivity and protect organ function?”
Why Stem Cell Therapy Thailand Is Being Discussed for SLE
The Interest Is Immune Modulation, Not Simple Tissue Replacement
When people hear the phrase stem cell therapy Thailand, they may imagine cells replacing damaged tissue. For SLE, that is not the most accurate explanation.
The more realistic discussion is immune modulation.
Umbilical cord-derived mesenchymal stem cells, or UC-MSCs, are studied because they may release bioactive signals, including cytokines, growth factors, extracellular vesicles, and other paracrine mediators. These signals may interact with immune cells and inflammatory pathways.
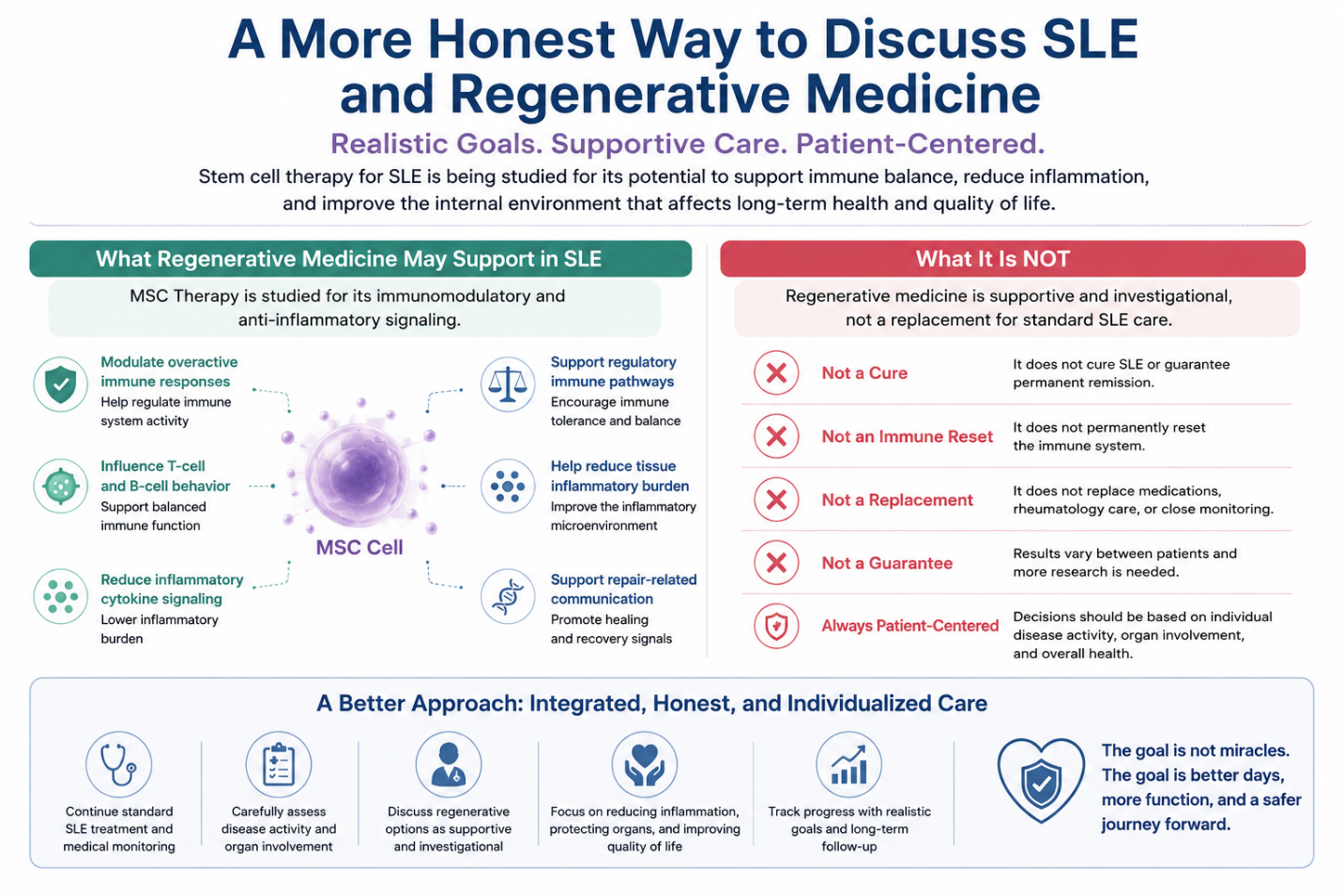
In SLE research, MSCs are being investigated for their potential to:
Modulate overactive immune responses
Influence T-cell and B-cell behavior
Reduce inflammatory cytokine signaling
Support regulatory immune pathways
Help reduce tissue inflammatory burden
Support repair-related communication in affected organs
This does not mean UC-MSCs “reset the immune system” permanently. It means researchers are studying whether MSC-based therapy may help create a less inflammatory immune environment in selected patients.
What Stem Cell News Says About SLE and Lupus Nephritis
Research Is Promising, But Still Not Final
In recent stem cell news in the context of autoimmune disease, attention is very often focused on MSCs for their immunomodulatory properties. Lupus nephritis, where immune activity impacts the kidneys in SLE is one of the best studied areas.
In conclusion, several clinical studies and reviews suggest that MSC therapy may exhibit preferential signals of a tentative efficacy in some SLE or lupus nephritis patients with amelioration of biomarkers reflecting disease activity, inflammatory burden as well as proteinuria; but also kidney-related outcomes. However, the results are not uniform across all of those studies.
The important point is balance. Despite continued research, conclusively clarifying these unanswered questions from small trials has proved more challenging and highlights the requirement for large-scale randomized controlled trials that employ standardized benchmarks regarding cell preparation, dosage protocols and nature of immunosuppression; as well as longer follow-up to permit sufficient time intervals beyond recurrent CT background levels in addition to more accurate patient selection.
Which is exactly why ethical clinics should NOT make claims about “treating lupus with stem cell therapy”, stopping all medications or curing by any means.
Who Might Be a Better Candidate for Discussion?
Patient Selection Matters More Than Hype
Not every SLE patient is the same. A patient with mild skin and joint symptoms is very different from a patient with active lupus nephritis, low complement levels, high anti-dsDNA, anemia, thrombocytopenia, or long-term organ involvement.
Before considering stem cell therapy Thailand for SLE, a physician should review:
Current SLE diagnosis and disease duration
Main organs involved
History of lupus nephritis
Current medications and response
Flare frequency
ANA, anti-dsDNA, complement C3/C4
ESR, CRP, CBC, kidney function, urine protein
Liver function and infection screening
Pregnancy plans, if relevant
History of severe infection or malignancy
Whether SLE is currently stable or actively flaring
A careful clinician should never accept an SLE patient based only on a short message or one symptom. Lupus requires a detailed review because immune suppression, infection risk, kidney status, and medication interactions all matter.
Stem Cell Therapy Should Not Replace Standard SLE Care
Rheumatology Care Remains the Foundation
Recent Overview of SLE Management. The current management approach in patients with SLE is generally aimed at achieving disease control, preventing flares, organ protection, and monitoring safety over time for long-term medication use. Hydroxychloroquine and/or corticosteroid taper based on disease severity, though some patients may require immunosuppressive therapy, biologics, or kidney-specific treatment.
But for patients who do not want these therapies in a clinical trial setting, stem cell therapy should be offered as an adjunct to the standard of care.
This matters because stopping lupus medication suddenly can be dangerous. SLE flares can involve the kidneys, brain, blood system, lungs, or heart. Any medication change should be made only by the patient’s treating physician.
Safety Questions Patients Should Ask Before Treatment
The Best Clinic Should Explain Both Possibilities and Limits
Patients searching for stem cell therapy Thailand should ask more than “How many cells will I receive?”
Important questions include:
What type of stem cells are used?
Are they UC-MSCs?
What is the donor screening process?
Are sterility, endotoxin, and viability tests performed?
Is infectious disease screening available?
Is the treatment reviewed by a physician?
Is SLE activity checked before treatment?
Are kidney function and urine protein reviewed?
What are the possible risks?
How will follow-up be monitored?
A responsible clinic should also explain when treatment may not be appropriate, especially during severe active flare, uncontrolled infection, unstable kidney disease, uncontrolled blood abnormalities, or when the patient needs urgent standard medical care.
A More Honest Way to Discuss SLE and Regenerative Medicine
The Goal Is Immune Balance, Not a Miracle Claim
For SLE, the most realistic conversation is not “Can stem cells cure lupus?” A better question is: “Can selected regenerative approaches support immune balance and reduce inflammatory burden as part of a broader medical plan?”
That is a more responsible and medically accurate way to discuss UC-MSCs.
The aims may be to assist immune regulation, heal the inflammatory environment, minimize flare burden in some patients, or even restore quality of life. In other cases, stem cell therapy might not even be indicated.
The optimal decision based on this evaluation will depend on disease activity, organ involvement, medication history, lab findings, and risk profile, but the final recommendation is also entirely dependent on the physician, who can be better positioned than an array.
Conclusion: What Patients Should Take From Stem Cell News
Stem cell research in SLE is advancing, particularly in MSC-based immune modulation and lupus nephritis. But stem cell news should be interpreted carefully. A headline is not the same as a clinical recommendation.
If you are a patient looking for stem cell therapy in Thailand, the safest and most practical approach is to go with clinics that treat SLE like other chronic diseases requiring care, review medical records scrupulously and describe what they do without hyperbole, all while promoting reasonable adjunctive support from standard rheumatology care.
SLE science does not chase the one breakthrough. It consists of a live, individualized plan to protect the patient long term: reducing flares and progression while protecting kidney function; controlling inflammation and organ damage in an honest, cautious manner whilst improving quality of life.
FAQ: Stem Cell Therapy Thailand for SLE
Can stem cell therapy cure SLE?
No. Stem cell therapy should not be presented as a cure for SLE. Current research is promising in some areas, especially immune modulation, but it remains investigational and results can vary.
Why are UC-MSCs being studied for SLE?
UC-MSCs are studied because they may release paracrine signals that influence immune cells, inflammatory cytokines, and regulatory immune pathways. The goal is immune modulation, not simple tissue replacement.
Is stem cell therapy useful for lupus nephritis?
Some studies have explored MSC therapy in lupus nephritis with encouraging but inconsistent results. More standardized clinical trials and long-term follow-up are still needed before it can be considered established care.
Can I stop lupus medication after stem cell therapy?
No responsible clinic should recommend stopping lupus medication without the treating rheumatologist’s approval. Stopping medication suddenly may increase the risk of flare or organ involvement.
What should SLE patients check before considering stem cell therapy Thailand?
Patients should prepare medical records, current medication lists, ANA, anti-dsDNA, complement C3/C4, CBC, ESR/CRP, kidney function, urine protein, liver function, infection screening, flare history, and details of organ involvement.