

When people search for stem cells and Parkinson stem cells, they are usually not looking for science fiction. Most are looking for a real answer to a very human question: do stem cells really work for Parkinson’s disease?
It is an understandable question. Parkinson´s disease is one progressive degenerative disorder that affects or robs your body of various types in function, such as movement and walking to facial expression balance speech sleep mood digestion independence. This neurodegenerative disease is closely related to the progressive reduction of dopaminergic producing neuronal cells in the brain, and many researchers have begun looking into migratory cell-based therapy as a possible alternative fix for either cellular replacement or support. It has only recently made the translation from theory to early stage human application in clinical research peaking with dopamine neuron replacement, but by no means does this mean that stem cells are yet proven as a cure for Parkinson’s.
The Better Question: Which Stem Cell, for Which Parkinson’s Goal?
The phrase stem cell sounds simple, but Parkinson’s research includes different approaches. Some are designed to replace dopamine-producing neurons. Others are being explored for inflammation balance, immune signaling, or neuroprotective support.
So, instead of asking only, “Do stem cells really work?” a more useful question is:
What kind of stem cell approach are we talking about, and what is it trying to do?
That question matters because Parkinson‘s stem cell research is not one single treatment. A general stem cell infusion is very different from a neurosurgical transplantation of lab-grown dopaminergic progenitor cells into the brain.
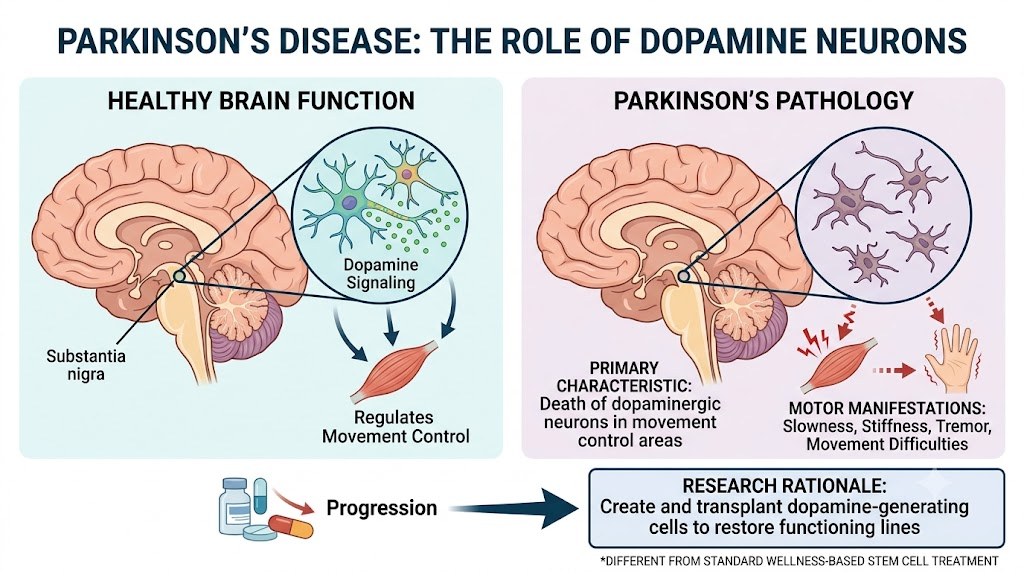
Parkinson’s Disease: Why Dopamine Neurons Matter
Now we know that Parkinsonian HMP is the most typical form of PD, and it gives rise mainly to motor manifestations (slowness, stiffness, tremor, one can move or ‘off’), including movement difficulties. One of the primary scientific characteristics is, in fact, the death of dopaminergic neurons within areas that regulate movement control. In the early stages, engagement in medical therapy can help alleviate symptoms; however, long-term treatment could become more challenging with disease progression.
That is where Parkinson’s stem cell research becomes so vital. Moreover, if scientists can safely create dopamine-generating cells and plant them where these neurons used to live, there could be a way forward towards bringing some sort of functioning lines back online. But that type of treatment is very particular. This is different from standard wellness-based stem cell treatment.
The Most Advanced Parkinson Stem Cell Direction: Dopamine Cell Replacement
The most exciting area of Parkinson‘s stem cell research is dopamine neuron replacement. In this model, scientists create dopaminergic progenitor cells from pluripotent stem cells, then transplant them into the brain area involved in Parkinson’s movement symptoms.
iPS Cell-Derived Dopaminergic Cells
At Kyoto University, a Phase I/II trial using plausibly dopaminergic progenitors derived from induced pluripotent stem cells in seven patients with Parkinson’s disease was reported. The study found no severe graft-specific adverse events, MRI indications of overgrowth, indirect evidence for local dopamine production, and motor-score improvements in some assessed patients. Describing their results as early-phase, the authors characterized them as indicating possible safety and clinical benefit.
Embryonic Stem Cell-Derived Dopaminergic Neurons
The other was a Phase I trial with bemdaneprocel, an investigational dopaminergic neuron progenitor product from human embryonic stem cells (hESC). A total of twelve patients were recruited, and one-year safety/tolerability objectives were met. Imaging indicated the graft was still present, and clinical endpoints improved or stabilized, more so with high-dose. But while this was still an early open-label trial, there was no conclusive proof that the therapy was ready to go for all Parkinson’s patients.
So, do stem cells really work?
The honest answer is: some stem cell approaches are showing early promise, but Parkinson’s stem cell therapy is not yet a simple, widely proven cure.
The early Dopamine replacement trials are encouraging. They not only show that stem-cell-derived dopamine cells survived under controlled clinical conditions in a few patients, but also evidence for them at least generating the potential to be able to generate dopaminergic signals. But these analyses stay small, extremely moderated and typical. This is not to say that just any stem cell treatment clinic will be able to provide the same result.
For broader MSC-based or supportive regenerative approaches, the discussion is different. Mesenchymal stem/stromal cells are usually studied for signaling, immune modulation, and inflammation balance rather than direct dopamine neuron replacement. These may be scientifically interesting, but they should not be marketed as the same as true dopamine cell transplantation.
Two Very Different Stem Cell Conversations
To make the topic clearer, Parkinson‘s stem cell care can be divided into two broad categories.
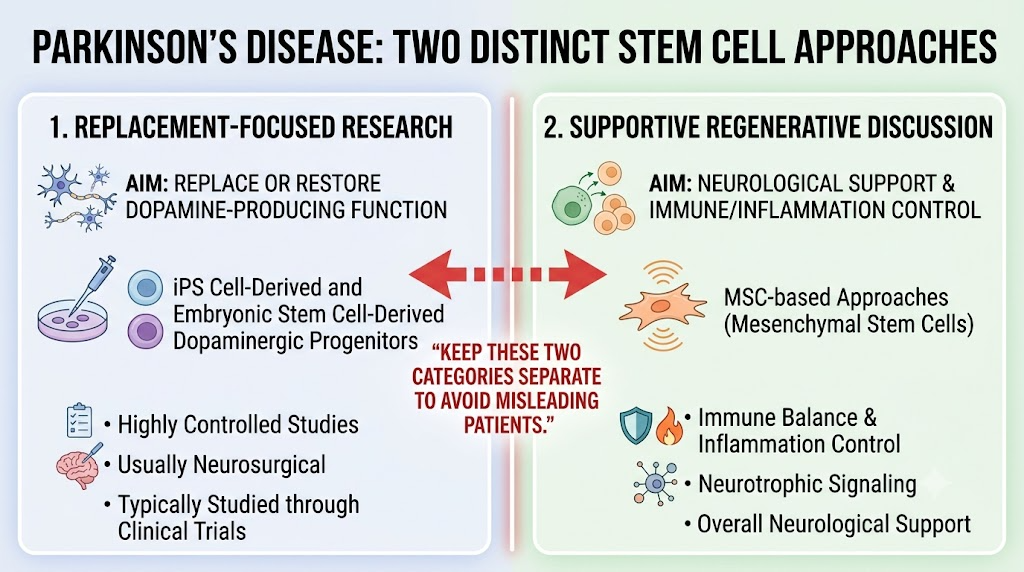
Replacement-Focused Research
This includes iPS cell-derived or embryonic stem cell-derived dopaminergic progenitors. The goal is to replace or restore dopamine-producing cell function. This is highly controlled, usually neurosurgical, and typically studied through clinical trials.
Supportive Regenerative Discussion
This may involve MSC-based approaches being explored for immune balance, inflammation control, neurotrophic signaling, or overall neurological support. This is not the same as replacing lost dopamine neurons.
A responsible article about stem cells and Parkinson’s should keep these two categories separate. Confusing them can mislead patients.
Why Parkinson Stem Cell Therapy Is Still Difficult
Parkinson’s disease is inherently complex and even with promising early trials. Motor symptoms may benefit from dopamine cell replacement, but Parkinson’s also has non-motor features including sleep disturbance, constipation and mood changes or cognitive change as well blood pressure regulation by autonomic nervous system centres affected in the disease process with later on muscular strutness and fatigue. Dopamine cell graft may not hit all facets of the disease.
There are also practical scientific questions:
Cell Survival
The transplanted cells must survive in the brain and connect functionally with existing circuits.
Safety
Researchers must monitor for tumor formation, graft overgrowth, immune reactions, dyskinesia, and other complications.
Patient Selection
Not every Parkinson’s patient may be a good candidate. Disease stage, age, symptom profile, medication response, and overall health all matter.
Long-Term Durability
Early improvement is important, but long-term follow-up is needed to understand whether benefits last.
What Patients Should Be Careful About
None of the regenerative medicine therapies has been approved by the U.S. FDA (Agency) for use in neurological diseases, including Parkinsons disease (PD). The FDA states that regenerative products marketed illegally pose serious risks, including the formation of tumors; neurological events (e.g., stroke); bacterial and viral infections; increased risk; and immune system reactions such as blood clots or lower than normal number(s)of red cells in the body due to destruction by antibodies after the tissue-derived stem cells from the fetus are used.
That is not to say, of course, that all stem cell treatments for Parkinson’s should be dismissed as a potential treatment. This also means you need to be wary whenever a clinic boasts that Parkinson’s stem cell treatment is certainly established, risk-free, or for everyone
What a Responsible Parkinson Stem Cell Clinic Should Explain
A clinic discussing stem cells for Parkinson’s should be able to explain the science in plain language.
What Cell Type Is Being Used?
Is it an MSC product, an iPS-derived dopaminergic progenitor, an embryonic stem cell-derived dopamine cell product, or something else?
What Is the Treatment Goal?
Is the goal dopamine replacement, inflammation support, neurotrophic signaling, wellness support, or rehabilitation support?
Is It Approved, Investigational, or Supportive?
This must be stated clearly. Early clinical research is not the same as routine approved treatment.
How Is Safety Monitored?
Patients should ask about cell testing, sterility, route of administration, physician supervision, imaging, follow-up, and adverse-event monitoring.
Will Standard Parkinson’s Care Continue?
A responsible clinic should not tell patients to stop neurologist care, medication, physiotherapy, exercise, speech therapy, or other standard support without specialist guidance.
The Human Side of the Question
When someone asks does stem cells really work, they may be asking from frustration, fear, or hope. They may have watched symptoms progress despite medication. They may be looking for something more than daily symptom control.
That hope deserves respect. But it also deserves honesty.
The best answer is not “yes, stem cells cure Parkinson’s.”The best answer is also not “no, nothing is happening.”
The real answer is more careful: Parkinson‘s stem cell research is advancing, especially in dopamine cell replacement, but most approaches remain investigational and must be evaluated through strong clinical evidence and long-term safety monitoring.
Conclusion
Another key aspect for the future of Parkinson’s research is stem cell science. Replacement of dopamine neurons is becoming a more attainable goal than previously envisioned, as demonstrated by early studies using iPS cell-derived and embryonic stem-cell derived dopaminergic cells. But it does not mean that all Parkinson’s stem cell treatments are proven, safe, and appropriate for every patient.
Solely answer to the question, stem cells really work for patients wondering, is that some methods of nerve cell replacement using stem cells in cautiously designed research studies appear preliminary, promising, but Parkinson’s disease-stem-cell-based therapy does not currently medial guarantee or substitute conventional neurological treatment.
The future may be exciting. Yet the best care in 2023 remains based on proper diagnosis, neurologist guidance driven by realistic expectations reinforced through rehabilitation and safety monitoring — as well as a clear-eyed understanding of what stem cell science can actually support at present vs. what it cannot yet deliver or promise?