

UC-MSCs and Duchenne Muscular Dystrophy with Physiotherapy: Supportive Stem Cell Therapy for Muscle Health and Functional Care
Treatment of Physiotherapy-Based Training Examples in UC-MSCs and DMD
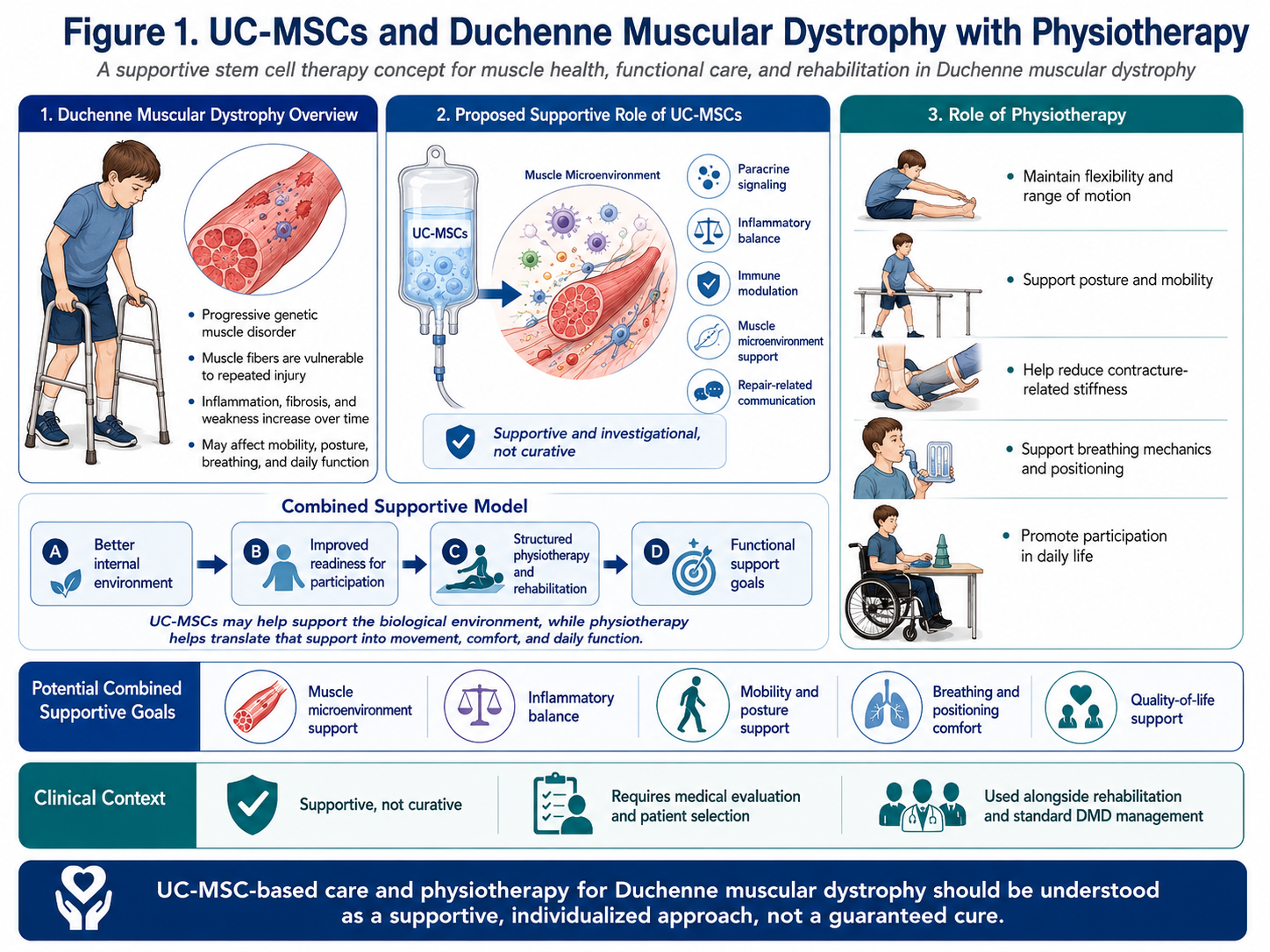
Duchenne muscular dystrophy, or DMD for short, is a genetic progressive muscle disease associated with changes of the DMD gene causing modifications in dystrophin (a protein that stabilizes muscle fibers during contraction). In the absence or decreased quantities of dystrophin, muscle fibers are less able to withstand small scale repeated injury and goes through inflammation, degeneration, and eventually replaced gradually by fibrotic or fatty tissue.
Since DMD affects both muscle biology and everyday function, a plan for supportive care should consider both sides of the equation. Potential roles of UC-MSC stem cell therapy as a pro-inflammatory or anti-inflammatory and microenvironment modulator (enhancing the muscle protective functions through paracrine signaling pathways), immune modulatory agent. Physiotherapy is the profession that takes those physical aspects of care and converts them to movement, flexibility, posture, breathing support, mobility preservation and independence in daily function.
The combination of UC-MSC transplantation with physiotherapy could represent a more integrated approach to supporting specific Duchenne muscular dystrophy patients.
What Are UC-MSCs in DMD Care?
The umbilical cord-derived mesenchymal stem/stromal cells (UC-MSCs) are newborn stem cell source in transplant immunology and regenerative medicine, frozen from the cells donated by donations of healthy birth. Adipose-derived mesenchymal stem cells are of interest in regenerative medicine due to their ability to secrete bioactive signals, including cytokines, growth factors, extracellular vesicles (without membrane receptors), and other paracrine factors.
In Duchenne muscular dystrophy, UC-MSCs are discussed more as a means of supporting host muscle repair indirectly than as a direct replacement of dystrophin or reformation of all damaged muscle. They are also possibly more valuable as means for cell-to-cell communication. UC-MSCs may contribute to controlling the environment surrounding the damaged muscle, mediating inflammatory balance and acting on repair-related signaling by paracrine signaling.
Applications for UC-MSCs in Duchenne muscular dystrophy
Supporting Inflammatory Balance
DMD is characterized by cycles of muscle injury and inflammation. This inflammatory stress may in time translate into muscle injury, fatigue, pain and fibrosis.
Signals released from UC-MSCs may act to moderate inflammatory pathways and/or support a less damaging environment for muscle. The aim is not to trick the disease into stopping altogether, but to create a stronger internal population bubble around fragile muscle fibers.
Supporting the Muscle Microenvironment
The microenvironment of muscle consists of muscle fibers, immune cells, blood vessels, connective tissue and extracellular matrix/repair-related cells. During the course of DMD, this environment becomes progressively more stressed.
Through paracrine signaling and tissue-supportive factors, UC-MSCs may aid to facilitate healthy communication within this microenvironment.
Supporting Repair-Related Signaling
On the other hand, UC-MSCs may secrete certain growth factors and extracellular vesicles (EVs) containing signaling molecules that could contribute to this type of communication during injury repair. This does not mean that UC-MSCs can correct the DMD gene or restore normal dystrophin production, but they might be able to deliver supportive biological signals in selected cases.
Supporting Quality-of-Life Goals
The clinical focus on UC-MSC-based support may seem broad in scope but tighter goals of improved muscle comfort, inflammatory buffering, proliferative signaling, and wellness have been established for select patients. This should always be used in conjunction with standard neuromuscular care, never instead of it.
Physiotherapy is vital in DMD
Importance of physiotherapy in patients with Duchenne muscular is a progressive disease which affects movement, posture, flexibility, breathing mechanics and functional independence. This could lead to tightness, contractures and then increase the risk of scoliosis, gait abnormalities, poor balance and a difficulty with functional movement (getting in/out bed or bath for example).
Physiotherapy targets preservation of range of motion, contracture prevention, mobility initiation support, positioning enhancement and comfort maintenance. Due to susceptibility of the DMD muscles to overwork and/or injury, physiotherapy should be gentle, ideally carefully structured, and medically guided.
Some Amazing Benefits of Physiotherapy for DMD
Staying Flexible and Full of Motion
Increased stiffness may decrease the range of motion: stretching and/or range-of-motion work can help mitigate these changes. This is significant since contractures can make moving, positioning, sitting, standing and caregiving more difficult.
Supporting Mobility and Functional Independence
Depending on the disease stage, physiotherapy may assist in optimally maintaining walking ability, transfers, posture, sitting balance and wheelchair position as well as functional daily movement skills for a longer period.
Supporting Respiratory and Postural Function
As the disease advances people with DMD can also find airway and respiratory muscles are involved resulting in postural difficulties. Respiratory physiotherapy may work in conjunction with a respiratory care service to aid breathing mechanism, chest wall movement, positioning and comfort.
Reducing Secondary Complications
As well as lessening immobility, tightness, poor positioning and discomfort, A good physiotherapy program may also help reduce complications related to reduced participation in daily life.
Reason to Introduce UC-MSCs To Physiotherapy For DMD?
The jointly administered UC-MSCs and physiotherapy regimen for Duchenne muscular dystrophy (DMD) can be conceptualized as a dual tiered supportive framework.
The role of UC-MSCs may play a supporting role for the inner biological environment.
They might favour inflammatory balance, immune modulation and paracrine signalling, communication within the muscle microenvironment.
Physiotherapy helps with functional movement and daily living
These keep flexibility, mobility, posture facilitation to breath support and for your ease of lifestyle.
This combination may be useful because DMD care is a mix of support that needs biological but also functional support. An internal environment that is more neutral may prime the body for improved participation, but physiotherapy provides progressive movement/exercise, stretching, positioning and everyday-life practice needed to support functional outcomes.
Potential Combined Benefits
An integrated UC-MSC cell therapy and physiotherapy strategy for DMD may assist with:
Muscle microenvironment balance
Inflammatory regulation
Repair-related signaling
Flexibility and range of motion
Mobility and posture support
Breathing and positioning comfort
Functional independence goals
QoL combined with ordinary therapy
It actually depends on the age of the subject, their personal status with DMD (how far along), level of mobility, function of respiratory system, condition of cardiac health and history with how responsive or compliant they will be with medications, exercise rehabilitation & nutrition.
Conclusion
Division of regenerative medicine: UC-MSCs and Duchenne muscular dystrophy movement supportive therapy coverage represents a conceptual bridge between biological signalling on the one hand, supported functional mobility in offspring (UCMSc) on the other. While UC-MSCs promote the aforementioned processes that aim to support inflammation regulation, immune modulation, and communication in the microenvironment of muscle contractile function, physiotherapy supports stretching flexibility, movement and posture breath support as well as ADL functions.
This combined strategy may provide a more comprehensive adjunctive approach for selected DMD patients. Finding others who believe this may take some time, and the intent is not to promise reversal of disease but rather to facilitate a care plan which adheres only as much/less than the individual and their physician wish; support in allowing the body, movement, comfort, spirituality-quality of life time-calculated.